
Content Page from Previous Semesters - For Reference Only
Note: This content was originally called "Disease and Development" and was written for a disease module, but it may fit best in a development module. -Seth Baum, 3 June 2011
Much of the discussion thus far has concentrated upon the ecological dimensions of human disease, either in terms of lyme disease or malaria. But human health is also shaped by social factors that contribute to disease vulnerabilities. It is therefore important to consider the ways that economic development is related human disease. Module 8 goes into detail on global development, but for our purposes here let’s think about development in terms of economic modernization, infrastructure investment and expanded access to certain commodities and services.
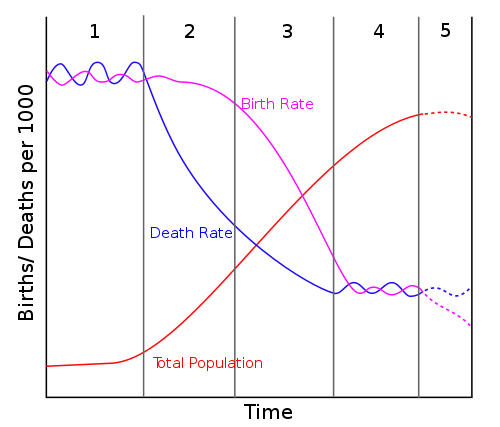
One way of thinking about development and disease is that development helps create the conditions that reduce vulnerabilities and transmission of disease. A clear example of this way of thinking is the demographic transition model, which is represented in Figure 5. Note that the stages are sometimes given these names: 1: preindustrial; 2: transitional; 3: transitional; 4: industrial.
{kind=link}
The demographic transition model was initially proposed in 1929 by demographer Warren Thompson. The model has four stages: pre-industrial, urbanizing/industrializing, mature industrial, and post-industrial. In the pre-industrial stage, crude birth rates and crude death rates remain close to each other keeping the population relatively level. During the urbanizing/industrializing stage, however, improvements in health care delivery and medicines, coupled with investments in sanitation and infrastructure, bring a sharp drop in the crude death rates. Note that crude birth rates remain roughly the same during this stage, thus prompting an increase in the population rate. During the mature industrial stage, crude death rates continue to decline, and it is theorized that economic development within the society bring incentives to bring the crude birth rates down slightly, however, the overall population continues to climb in an exponential j-curve. In the post-industrial stage, the population growth begins to level off because the crude birth rates have reduced to closely follow the crude death rates.
In essence, the demographic transition model argues for economic development to help reduce crude death rates. It is assumed that access to medicines, safe drinking water and sanitation, and information about disease, will help improve human health. There is a behavioral component to this way of thinking, in that it assumes that people change their decision-making because they have access to information or other opportunities that reduce certain behaviors.
There is some evidence that the demographic transition model is effective in understanding the relationships between economic development and human population. Rather than assess crude birth rates and crude death rates, let’s now look at fertility rates. The fertility rate is the estimate of the average number of children that would be born to a woman in a country over the course of her lifetime, assuming she lives a full and healthy life. In order for a country’s population to stay steady (minus immigration), the fertility rate needs to be 2.1, which replaces the parents and accounts for mortality due to unexpected causes. Whether the demographic transition is correct or not, there are clear associations between economic development and fertility rate. This can be seen by assessing some national fertility rates from 2008/2009 (Source: World Bank.)
The table seems to support the idea that economic development is tied to a reduction in the population due to natural reproduction. Countries classified as “industrial” (such as Australia, Italy, Japan, Switzerland, and the United States) have fertility rates at, or below, the replacement level of 2.1 In fact, the “population challenge” for many of these countries is ensuring the population continues to grow to ensure a future labor force and tax base to support government programs. Countries that are underdeveloped or developing (such as Burkina Faso, Chad, India, and Zambia) have higher fertility rates. More important than the fertility rate is that many of the countries in the developing world lack basic health care services and infrastructure that ensure a healthy quality of life. Human populations in these countries are therefore more vulnerable to certain diseases over the course of their lifetimes. This has contributed to the insistence by development organizations and some public health experts that the elimination of poverty is the most important consideration in reducing the spread and impact of human diseases.